Pretest Newborn
CHARGE
coloboma
heart defect
atresia choanae
retardation, growth: linear growth tends to decline by late infancy
genital hypoplasia
ear anomalies/deafness
Diabetic Mother Infant
Infants of diabetic mothers have an increased chance of congenital heart disease (transposition, failure to twist), caudal regression syndrome, and a small left colon. Besides, they are large-for-gestation age and have a number of biochemical abnormalities such as hypoglycemia or hypocalcemia.
Down Syndrome
protruding tongue
Brushfield spots
redundant neck skin
mental retardation
brachycephaly
upslanting palpebral fissures
epicanthal folds
flat face
small ears
cardiac abnormalities (especially ventricular septal defect or endocardial Cushing defect)
palmar creases
clinodactyly of the fifth digit.
Hyperbilirubin
Sulfisoxazole, ceftriaxone and other drugs compete with bilirubin for binding sites on albumin
nonesterified fatty acids, which are elevated during cold stress compete with bilirubin for albumin-binding sites.
Metabolic acidosis also reduces binding of bilirubin. Increased hydrogen competes with bilirubin for albumin.
sepsis interrupts the blood–brain barrier, thus allowing diffusion of bilirubin into the brain.
Administration of phenobarbital has been used to induce glucuronyl transferase in newborn infants and canreduce, rather than exacerbate, neonatal jaundice.
Varicella
onset of varicella < 5 days before delivery: VZIG to infant immediately after delivery
onset of varicella < 2 days after delivery: VZIG
no VZIG or isolation if > 2 days
Breastfeeding CI
Active pulmonary tuberculosis and HIV are two examples of infectious contraindications in developed countries, as well as malaria, typhoid fever, and septicemia.
In underdeveloped countries, the risk of infectious diarrhea due to use of contaminated water to mix formula or the unavailability of formula can preclude this recommendation.
Meds: antineoplastic agents, lithium, cyclosporin, illicit drugs including cocaine and heroin, amphetamines, ergotamines, and bromocriptine (which suppresses lactation).
Mothers with mastitis can continue to breast-feed; frequent feedings may help the condition by preventing engorgement.
Apt Test
differentiates fetal from adult hemoglobin in a bloody specimen.
The test is based upon the finding that fetal hemoglobin is alkali resistant, while adult hemoglobin will convert to hematin upon exposure to alkali.,
Catch up feeding
Breast milk has much less calcium (and phosphorus) than do commercial formulas
ABO and Coombs
In comparison with hemolytic disease caused by Rh incompatibility, where it is usually strongly positive, major blood-group incompatibility is often associated with a direct Coombs test that is frequently weakly positive.
Infant tachypnea
Within minutes of delivery, the infants are likely to become pale or blue and their body temperatures will drop. In order to bring body temperature back to normal, they must increase their metabolic rate; ventilation, in turn, must increase proportionally to ensure an adequate oxygen supply. Because a preterm infant is likely to have respiratory problems and be unable to oxygenate adequately, lactate can accumulate and lead to a metabolic acidosis. Infants rarely shiver in response to a need to increase heat production.
SGA
Small-for-dates infants are subject to a different set of complications than preterm infants whose size is appropriate for gestational age. The small-for-dates infants have a higher incidence of major congenital anomalies and are at increased risk for future growth retardation, especially if length and head circumference as well as weight are small for gestational age.
Also more common are neonatal asphyxia and the meconium aspiration syndrome, which can lead to pneumothorax, pneumomediastinum, or pulmonary hemorrhage. These, rather than hyaline membrane disease, are the major pulmonary problems in small-for-gestational-age infants.
Apnea
path:
Periods of apnea are generally thought to be secondary to an incompletely developed respiratory center, particularly when they are seen, as is common, associated with prematurity.
Idiopathic apnea is common in premature infants but is not expected in the full-term newborn. When apnea occurs in the term infant, there is almost always an identifiable cause. Sepsis, gastroesophageal reflux, congenital heart disease, seizures, hypoglycemia, and airway obstruction can cause apnea in term newborns.
symptoms: characterized by an absence of respirations for more than 20 seconds and may be accompanied by bradycardia and cyanosis.
Other, less common, explanations for central apnea include congenital central hypoventilation syndrome (formerly known as Ondine’s curse), Arnold-Chiari malformations, and congenital infections.
Periodic breathing, a common pattern of respiration in low-birth-weight babies, is characterized by recurrent breathing pauses of 3 to 10 seconds.
Galactosemia
Early treatment is essential and consists of galactose avoidance (soy or casein hydrolysate infant formula).
Clavicle fracture
While some fractures are identified at birth, others may not be identified until callus formation (tender bump at shoulder) is noted at about a week of age. Clavicular fracture may happen in any delivery, although there is higher risk with large-for-gestational-age infants. Initial presentation of a fractured clavicle may include a pseudoparalysis, in which the infant refuses to move the ipsilateral arm, mimicking an Erb-Duchenne paralysis.
Maternal Toxemia
Aka: pre-eclampsia
pt: SGA baby. Pregnancy-induced hypertension can produce a decrease in uteroplacental blood flow and areas of placental infarction. This can result in fetal nutritional deprivation and intermittent fetal hypoxemia, with a decrease in glycogen storage and a relative erythrocytosis, respectively. Labs: Hence, neonatal hypoglycemia and polycythemia are common clinical findings in these infants.
A persistent venous hematocrit of greater than 65% in a neonate is regarded as polycythemia and will be accompanied by an increase in blood viscosity.
symptoms: Manifestations of the “hyperviscosity syndrome” include tremulousness or jitteriness that can progress to seizure activity because of sludging of blood in the cerebral microcirculation or frank thrombus formation, renal vein thrombosis, necrotizing enterocolitis, and tachypnea.
treatment: Simple phlebotomy, while decreasing blood volume, will also decrease systemic arterial pressure and thus increase viscosity (based on Poiseuille law of flow). Therapy by partial exchange transfusion with saline or lactated Ringer solution is preferred.
Meconium Aspiration
Infants who are postmature (more than 42 weeks’ gestation) and show evidence of chronic placental insufficiency (low birth weight for gestational age and wasted appearance) have a higher than average chance of being asphyxiated, and passage of meconium into the amniotic fluid thus places these infants at risk for meconium aspiration.
Erythromycin
However, asymptomatic infants born to chlamydia-positive mothers are not routinely treated with oral antibiotics at birth as prophylaxis, but rather watched closely for signs of infection, due to an increased incidence of hypertrophic pyloric stenosis among neonates having received erythromycin.
NRDS Shunt
In this disease, lung compliance is reduced; lung volume is also reduced, and a significant right-to-left shunt of blood can occur. Some of the shunt can result from a patent ductus arteriosus or foramen ovale, and some can be due to shunting within the lung. Minute ventilation is higher than normal, and affected infants must work harder in order to sustain adequate respiration.
TEF
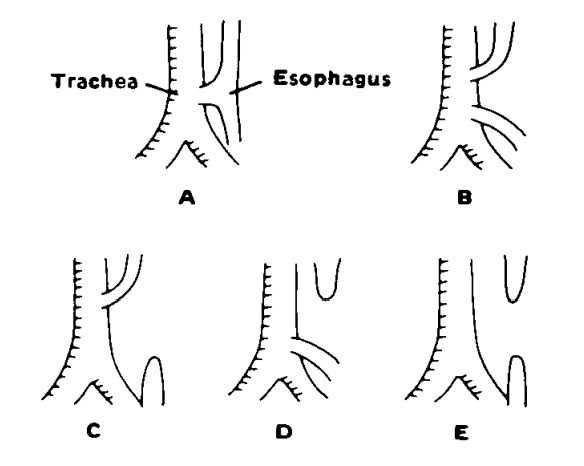
Abdominal distention, choking, drooling, and coughing associated with feedings are symptoms of esophageal anomalies. The anomaly illustrated by D is the most common; that of A can be diagnosed after repeated episodes of pneumonia. The anomalies in E and C are associated with all the same symptoms except abdominal distention, which cannot develop because air cannot enter the gastrointestinal tract. B and C are the least common; in these, the upper esophageal segment is connected directly to the trachea, and massive entry of fluid into the lungs occurs.
Beta blocker teratogenicity
May cause growth retardation when given throughout pregnancy, diminishes the ability of an asphyxiated infant to increase heart rate and cardiac output. It has also been associated with hypoglycemia and apnea.,
Goat milk
inadequate iron and folate
brucellosis if unpasteurized
Cleft lip and palate
Although affected infants are likely to have feeding problems initially, these problems usually can be overcome by feeding in a propped-up position and using special nipples.
Complications include recurrent otitis media and hearing loss as well as speech defects, which may be present despite good anatomic closure.
Repair of a cleft lip usually is performed within the first 2 to 3 months of life; the palate is repaired later, usually between the ages of 6 months and 5 years.
Polydactyl
If black: normal. If white: check for other problems. Some syndromes that are associated with polydactyly are trisomy 13, Rubinstein-Taybi syndrome, Meckel-Gruber syndrome, and Ellis-van Creveld syndrome
Waardenburg
path: autosomal dominant trait with variable penetrance.
symptoms: It includes, in decreasing order of frequency, the following anomalies: lateral displacement of the medial canthi, broad nasal bridge, medial hyperplasia of the eyebrows, partial albinism commonly expressed by a white forelock or heterochromia (or both), and deafness in 20% of cases.,


Sturge Weber
The malformatio nalso involves the meninges and results in atrophy to the underlying cerebral cortex. The damage is manifested clinically by grand mal seizures, mental deficiency, and hemiparesis or hemianopsia on the contralateral side.,
Last updated