Tremors
Hypokinetic
Parkinson

dopamine inhibits GABA that inhibits movement
Ach stimulates GABA that inhibits ovement
Parkinson: no D2 from substantia niagra
risk increases with welders: indoor, Mg heavy metal consumption
Symptoms
Criteria:
Bradykinesia: everything slower. Finger taps, mask liked faces, migrographia
cogwheel rigidity
resting tremor, only 75% of patients: pill rolling. Tremor comes back when put hands up
gait instability
symptoms worse with stress/anxiety, decreased sleep, caffeine, after exercise
Dysutonomia: conspitation most common, depression, hypotension
Diagnosis
Clinical, no imaging
Treatment
Ach-i for young people. Do not use amantadine
COMT, MAO-B, L-DOPA/carbidopa, dopamine agonists
dopamine agonist SE: impulse control, nausea, VH, leg edema, hypersomnolence
worse parkinson with antidopamine drugs: reserpine, antipsychotics, anti emetics
Management, pt comes in:
if <70, functional: start with dopamine agonists
if > 70, or dysfunctional: L-DOPA/Carbidopa, MAO/COMT adjunct
DBS if medications fail
Parkinson's Plus
bilateral, fall in 1st 2 years
Multiple Systems Atrophy
Dysautonomia: sweating, hypotension, bladder function
Shy Drager: MSA-P, Parkinson like
Olivopontocerebellar atrophy: MSA-C, cerebellar like
treatment is aimed at intravascular volume expansion with fludrocortisone, salt supplementation, alpha-adrenergic agonists, and application of constrictive garments to the lower body.
Progressive Supranuclear Palsy
Bilateral, early falls, supranuclear palsy: saccade length/velocity down
Corticobasal Degeneration/Syndrome
bilateral, early falls, cortical signs: apraxia, aphasia, blindness, acalculus
Lewy Body Dementia
bilateral, early falls, VH
Hyperkinetic

Movementents
athetosis: smalest amplitude, velocity
Chorea: medium
ballism: largest amplitude, velocity
Essential Tremor
path: familial
symptoms: tremor with movement/use, no resting. Same tremor whole way. Hand, neck, voice, no leg symptoms. Handwriting large and straight
pt: male, 40-60
treatment: propranolol, primidone, alcohol, no response to levodopa
Essential tremor is exacerbated by goal-directed movements that involve extension of the arms (e.g. finger-to-nose testing, drinking from a cup).
Essential tremor is most often inherited in an autosomal dominant manner.
Essential tremor is relieved by small amounts of alcohol and is usually not aggravated by caffeine.
First-line treatments for patients with essential tremor include propranolol or primidone, an anticonvulsant.
Patients with essential tremor that fail pharmacologic therapy are candidates for deep brain stimulation or thalamotomy.
Intention Tremor
path: cerebellar dysfunction
symptoms: no tremor at rest, tremor with movement, worse closer with target
diagnosis: clinically
treatment: no treatment
Physiologic Tremor
Physiologic tremor is a benign tremor with low amplitude and high frequency (12-14 Hz) that is not visible under ordinary conditions. Unlike the resting tremor seen in this patient, physiologic tremors are postural tremors (eg, holding arms outstretched) and infrequently occur with action. Physiologic tremors are usually worsened with emotional or physical stress, toxic/metabolic derangements, caffeine, or drug withdrawal.
Orthostatic Tremors
Orthostatic tremor is a postural tremor considered to be a variant of essential tremor. Orthostatic tremor occurs in the legs immediately on standing and is relieved by sitting down. It is usually high frequency (14-18 Hz) without other clinical signs or symptoms.
Huntingtons Chorea
path: CAG repeats, anticipation, AD
symptoms: chorea (ballistic, uncontrolled movement), depression, psychosis
diagnosis: clinical
treatment: none
Restless leg
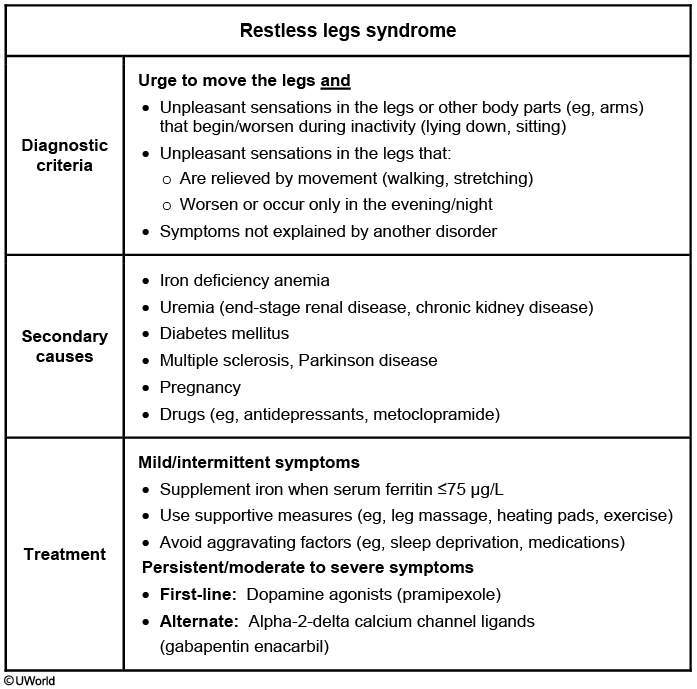
causes
idiopathic, iron deficiency, end stage renal, pregnancy, birth control
diagnosis
noncomfort sensation: like migraines in legs, not on surface/paresthesia
worse with rest
better with movement
worse at night
treatment
augmentation: worse with dopamine treatment. No augmentation with gabapentin
Other Movements
Chorea
Chorea is a hyperkinetic movement characterized by rapid, unpredictable, involuntary movements of the limbs, often described as"dance-like". Chorea results from an imbalance between indirect and direct pathways in the basal ganglia, leading to increased dopaminergic activity.
Diseases associated with chorea include:
Hyperthyroidism
Stroke
Huntington disease
Systemic lupus erythematosus
Levodopa use
Rheumatic fever
Lesch-Nyhan syndrome
Dopamine receptor blockers are the most effective agents to reduce the severity of choric movements. In some patients the use of second generation antipsychotics can also decrease chorea.
Athetosis
Athetosis is characterized by writhing, snake-like movement in extremities, especially the fingers.
Diseases associated with athetosis include:
Cerebral palsy
Encephalopathy
Huntington’s disease
Wilson’s disease
Treatment of athetosis involves treating the underlying disorder as no one drug has been shown to reduce symptoms.
Dystonia
Dystonia is characterized by sustained proximal limb and trunk contractions.
Diseases associated with dystonia include:
Wilson’s disease
Parkinson’s disease
Huntington’s disease
Encephalitis
Neuroleptic use, which is itself associated with tardive dyskinesia
Treatment options for dystonia include:
Carbidopa
Levodopa
Botulinum toxin
Treatment of the underlying disorder
Hemiballism
Hemiballismus is characterized by flinging of a proximal extremity only occurring on one side.
Hemiballismus is typically associated with a lacunar stroke affecting thecontralateral subthalamic nucleus.
Hemiballismus is treated with haloperidol.
Tics
Tics are characterized by repetitive brief involuntary movements or sounds.
Diseases associated with tics include:
Tourette syndrome
Obsessive-compulsive disorder
ADHD
Treatment options for tics include:
Tetrabenazine (first-line)
Antipsychotics: risperidone, fluphenazine, pimozide , haloperidol
Alpha 2 agonists: clonidine, guanfacine
Last updated