18 TB
Overview
Characteristics

Infection

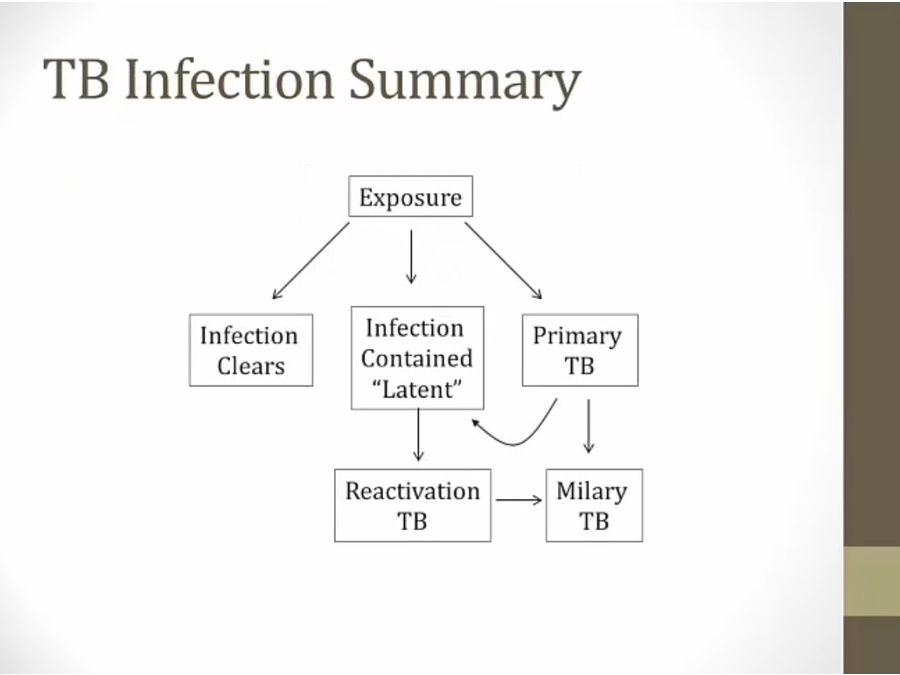
Primary

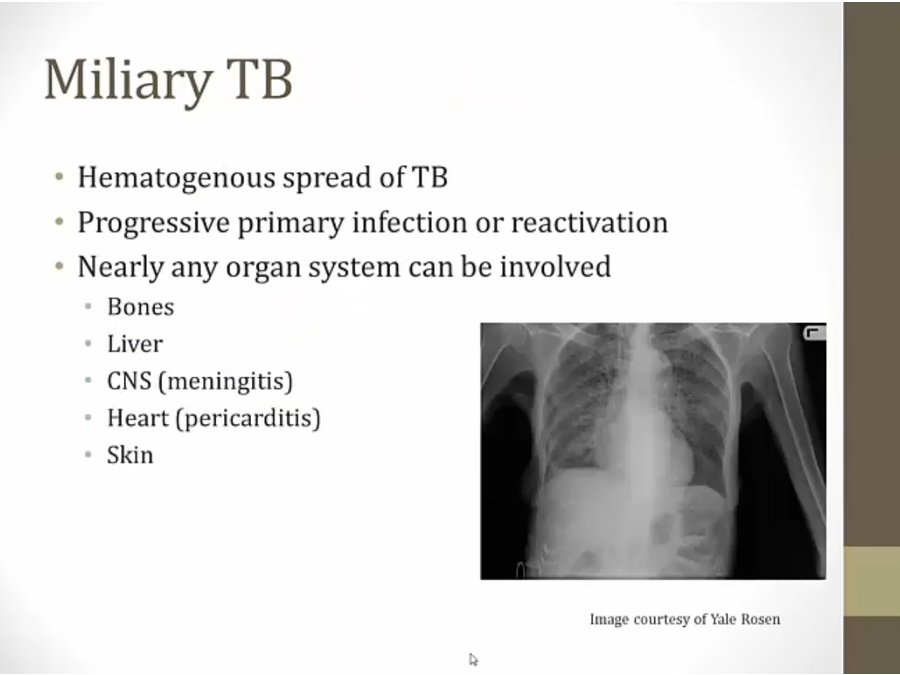
Miliary TB
Reactivated TB

Aspergilloma
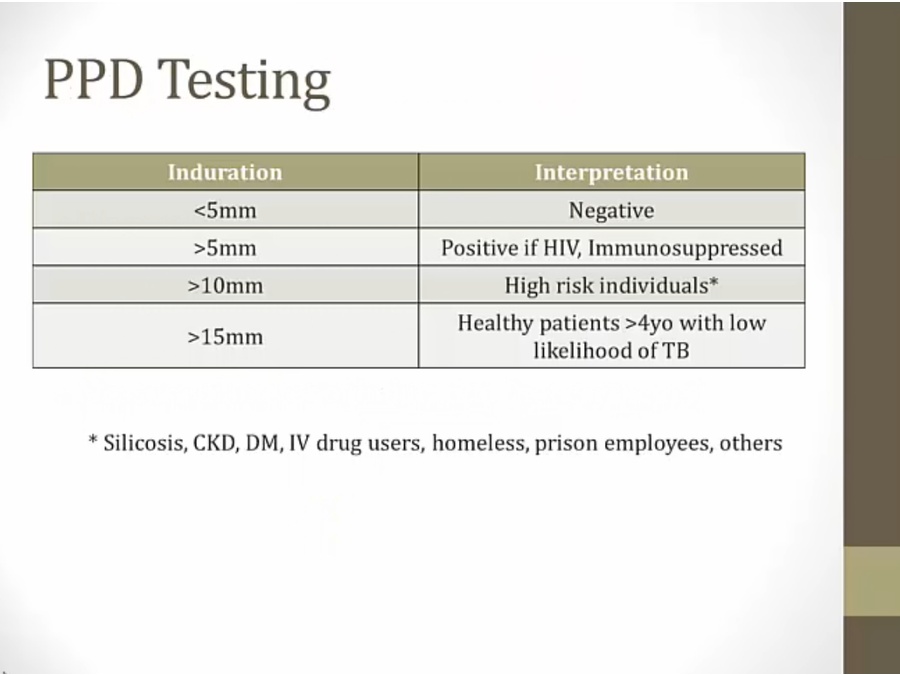
Diagnosis
Treatment

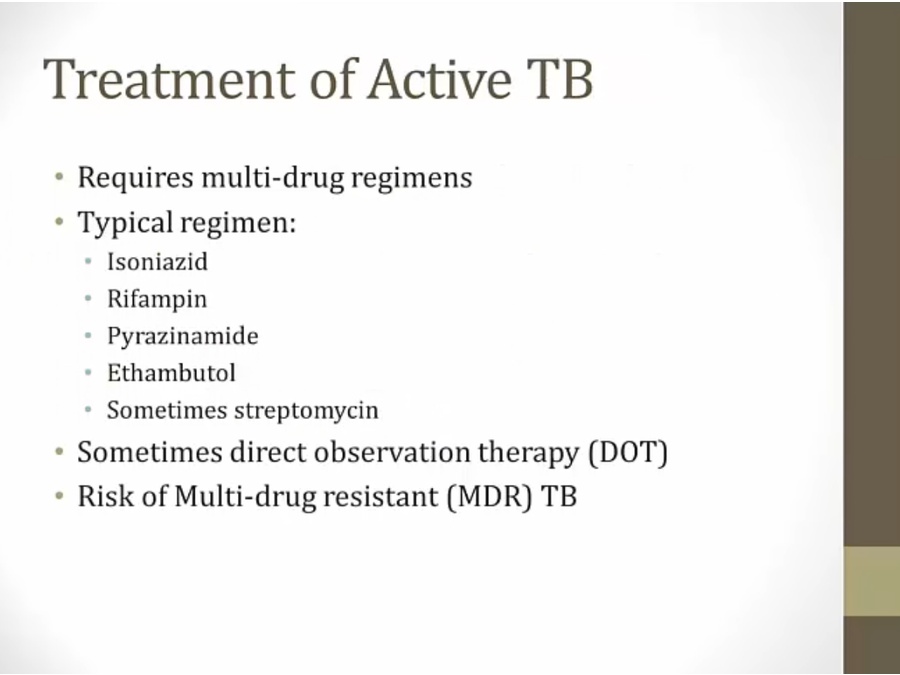
INH
Rifampin

Pyrazinamide
Ethambutol
Streptomycin

Last updated