15 EKG Others
AFIB
Pathogenesis
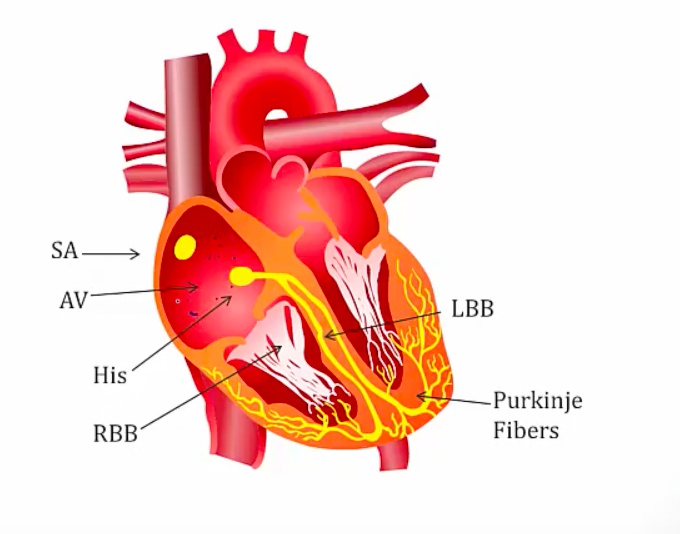
small depolarization occuring in atrium irregularly, some reach AV and generate QRS, others reach AV during refractory
result: random QRS
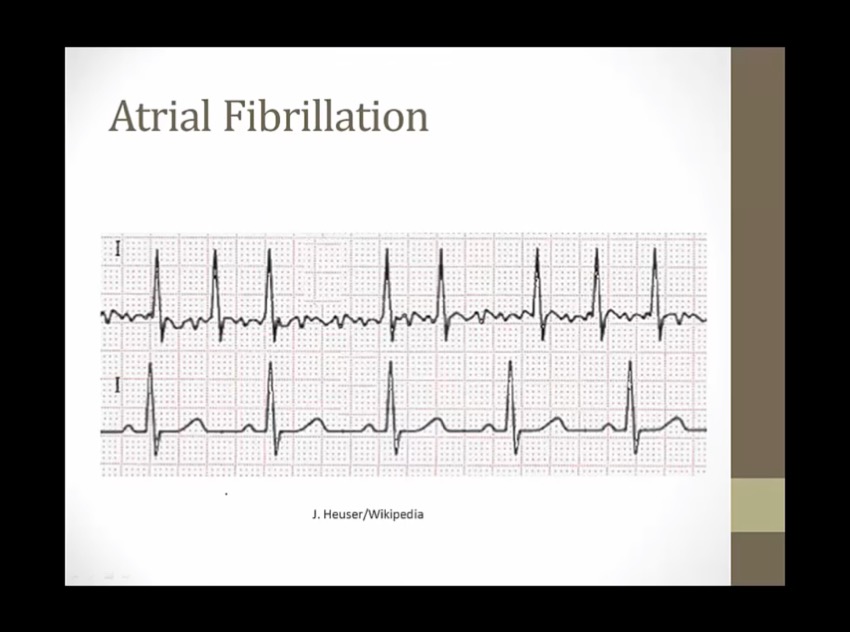
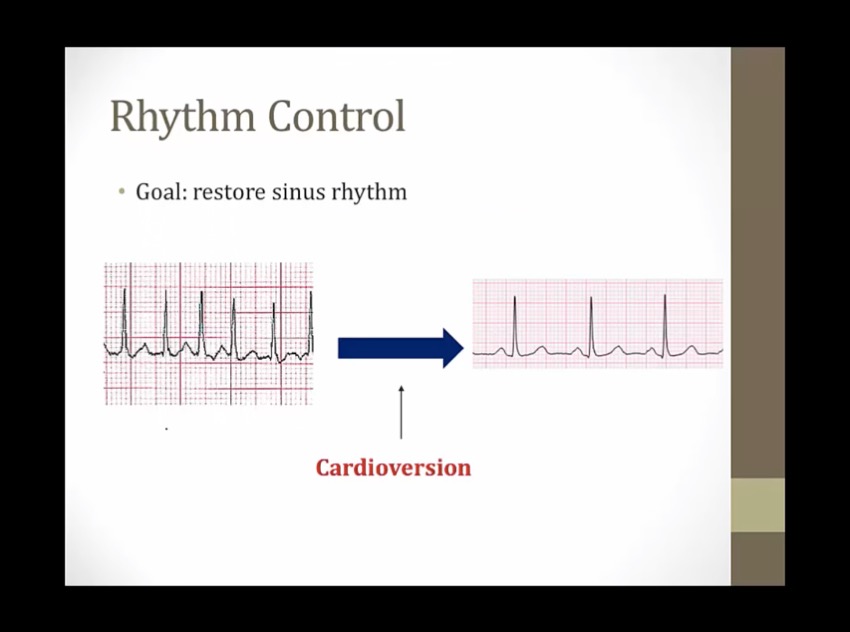
bottom: normal
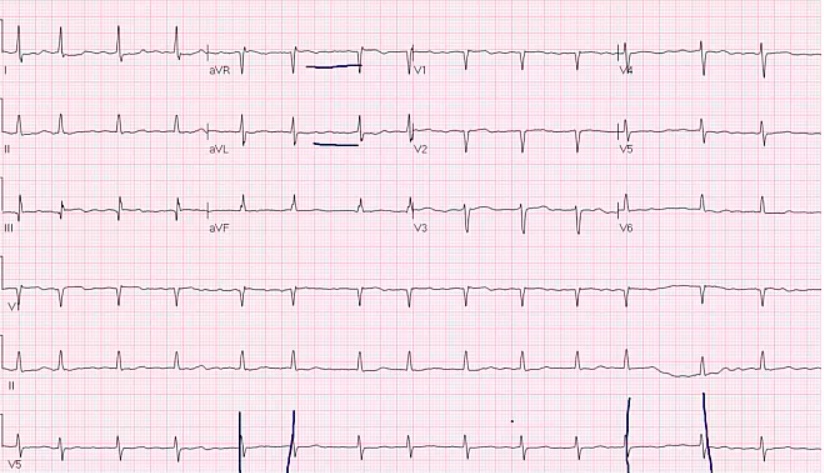
top: AFIB, bumps before QRS but not organized regular bumps. QRS at irregularly irregular (irregular and no pattern to the irregularity)

bumps are actually T waves, not P
Types and Symptoms
young pts: healthy AV node, fast
aortic stenosis: need preload to generate enough output to get past stenosis
stiff ventricles: need atrial kick to fill the stiff ventricles
can see cardiogenic shock during Afib
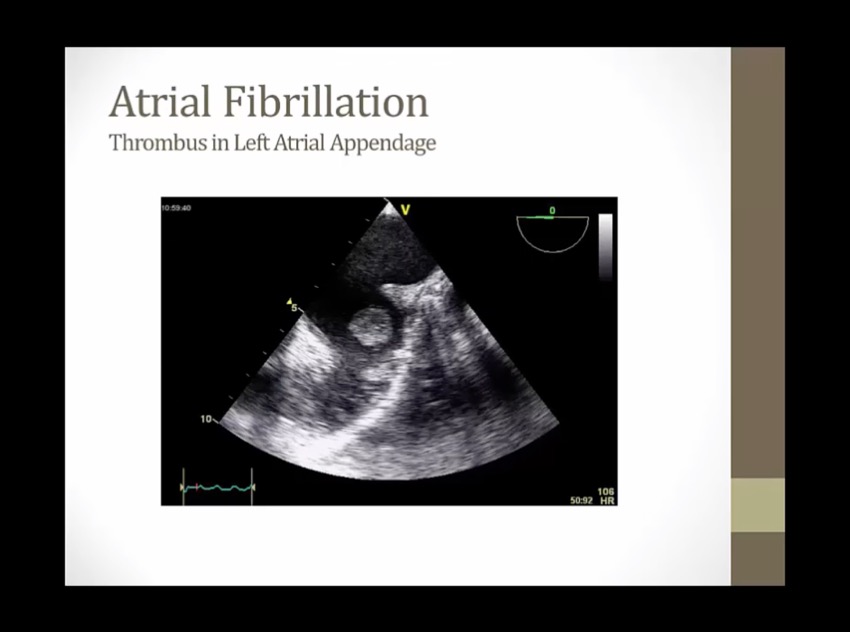
arrhythmia itself usually not life threatening, thrombus is
blood flow slower during afib
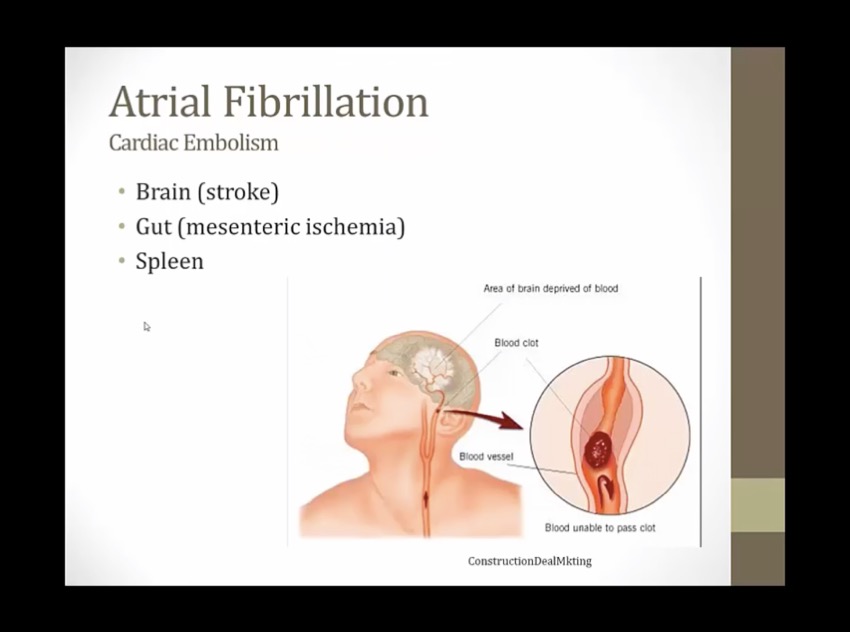
splenic infarct
when both mitral stenosis and afib, refractory to treatment
many drugs only test with pts with non-valvular afib
HR has to be rapid to cause cardiomyopathy
untreated afib for weeks: EF decline
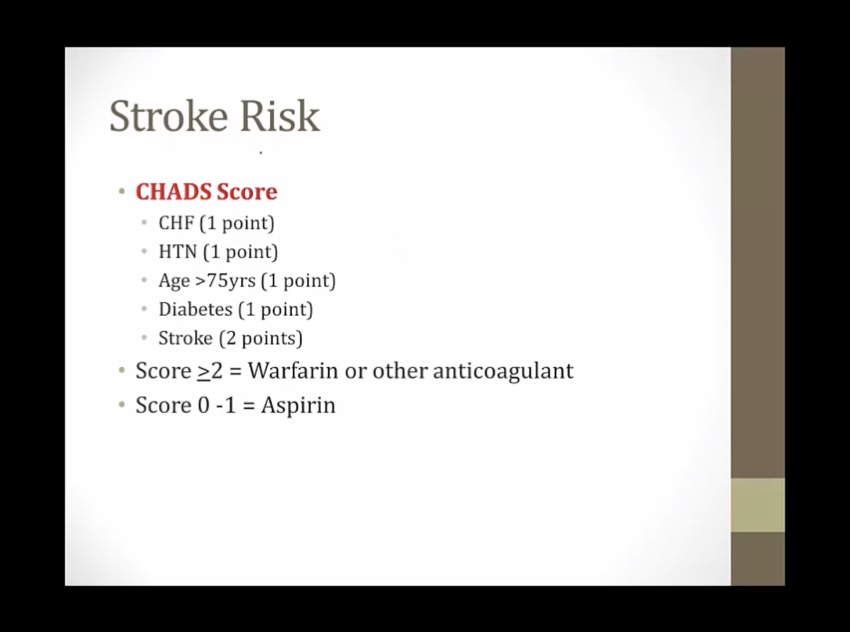
Risks
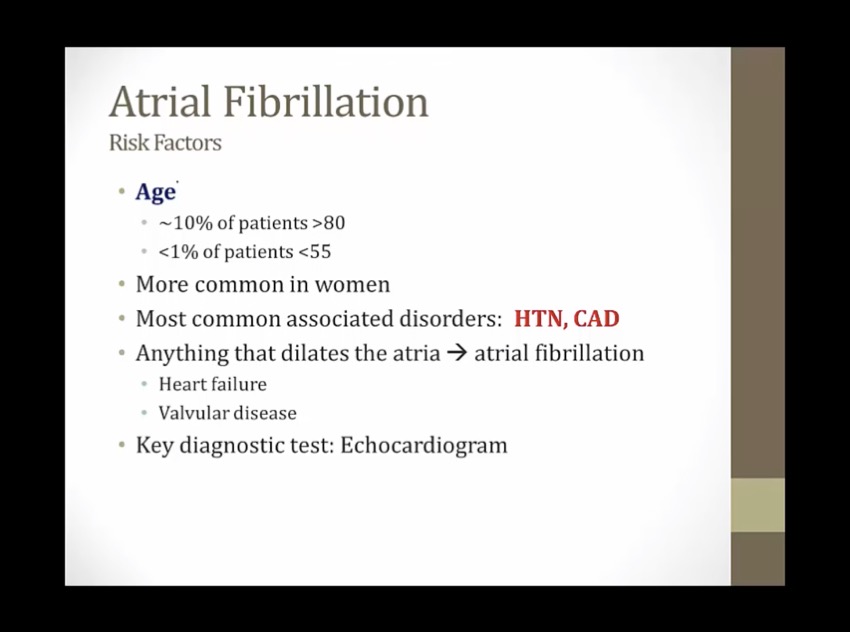
HF: high pressures in RA and RV
echocardiogram: key test, determine if enlarged heart
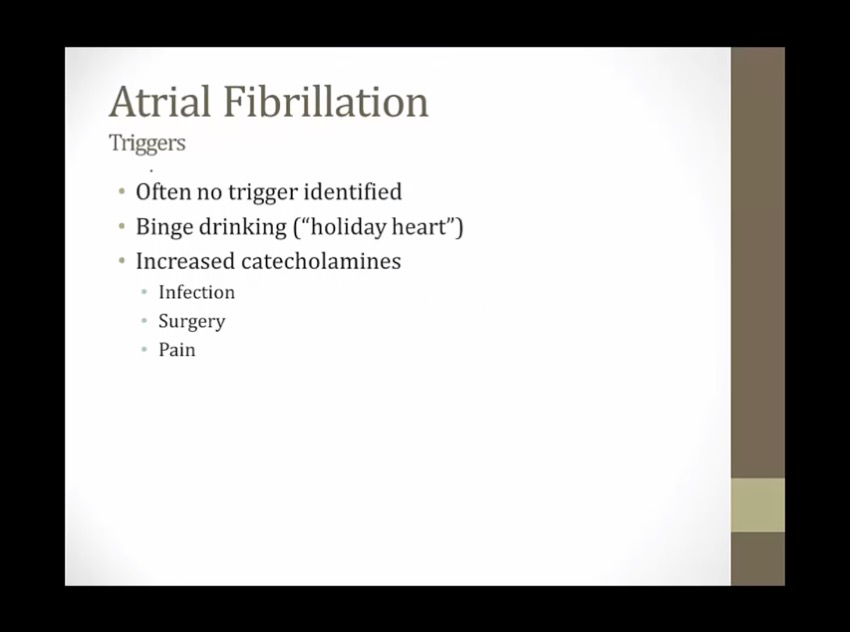
elderly with PNA
pain after trauma
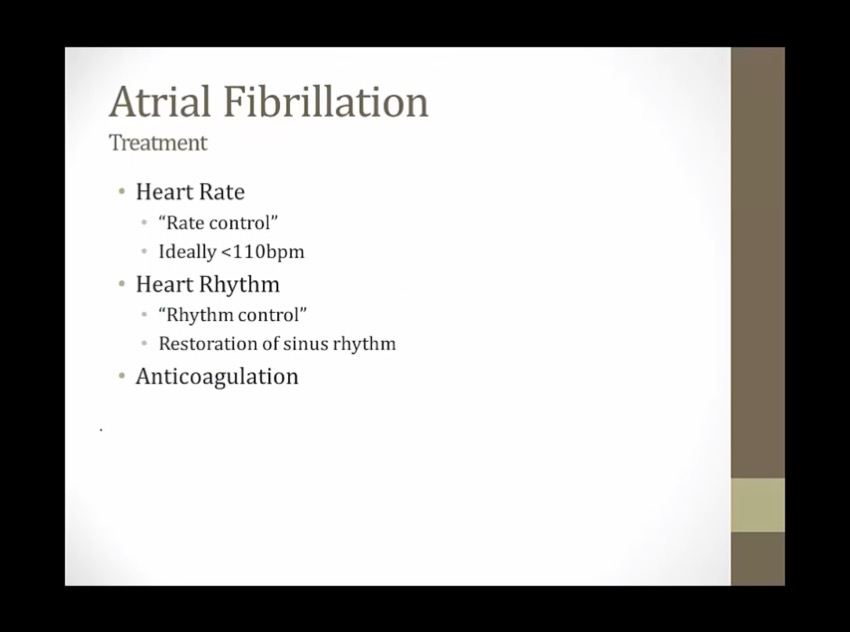
Treatment
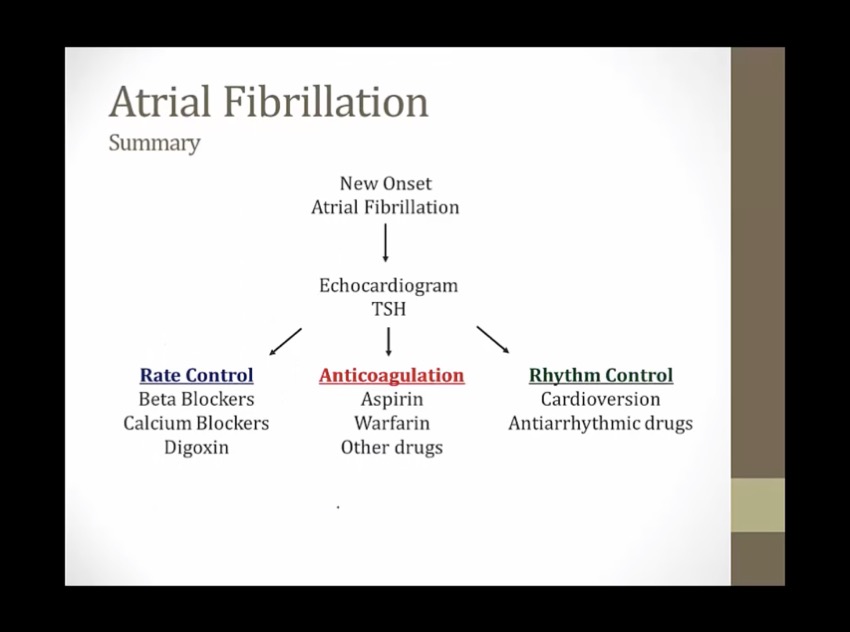
echo: exclude structural heart disease
rate control first
surgery last resort
Rate
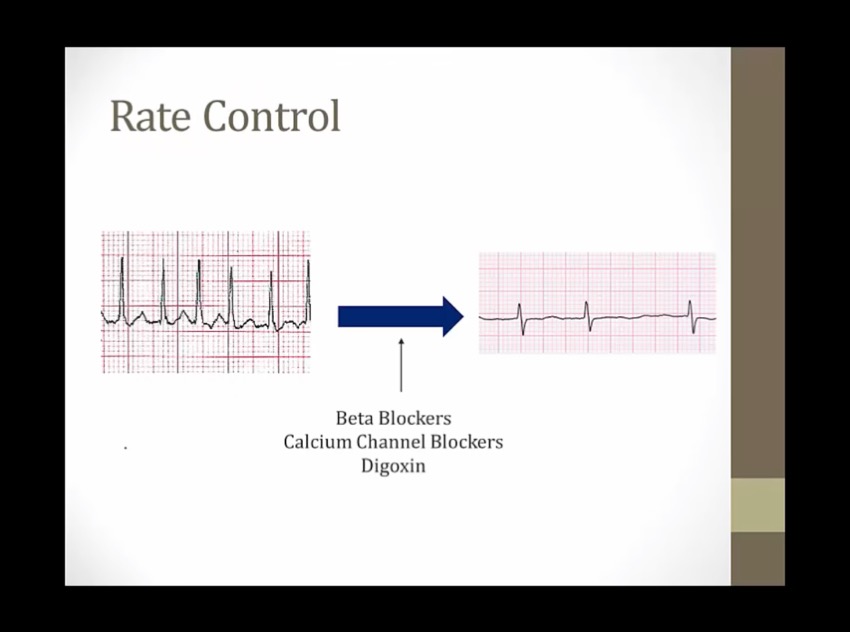
1st thing to do after pt present with afib and fast HR: decrease HR
will still have irregular rhythm, but good HR
pt will feel much better with slower HR
for elderly, usually all that's done
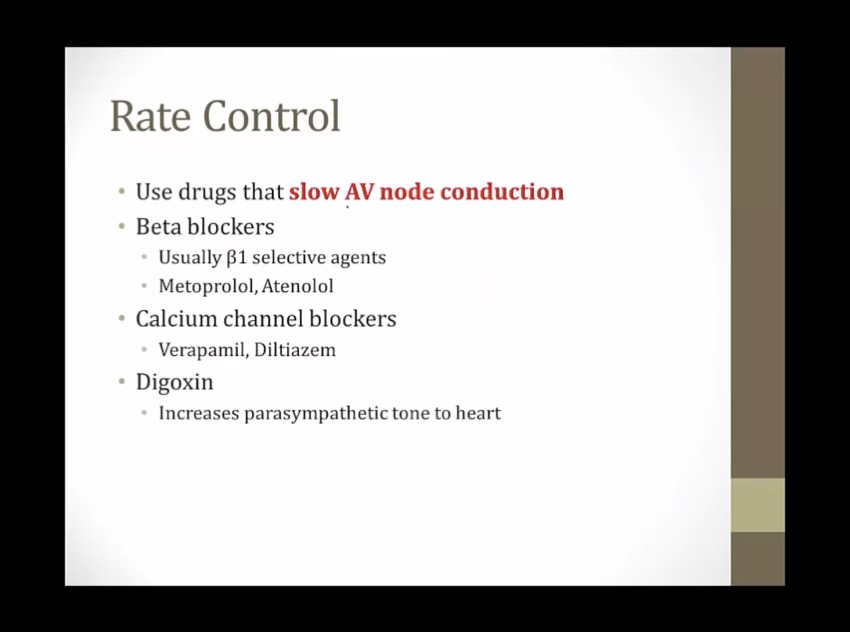

Irregularly irregular static: beta blockers are useful in atrial fibrillation and flutter
Metronome: beta blockers prevent rapid ventricular response in atrial fibrillation and flutter ("rate control") (increase AV node refractory period, slow ventricular response rate)

Illuminated top: non-dihydropyridine CCBs treat supraventricular arrhythmias (e.g. atrial fibrillation with RVR)
Irregularly irregular signal: non-dihydropyridine CCBs are useful in atrial fibrillation (and flutter)
Metronome: non-dihydropyridines prevent rapid ventricular response in atrial fibrillation and flutter ("rate control")

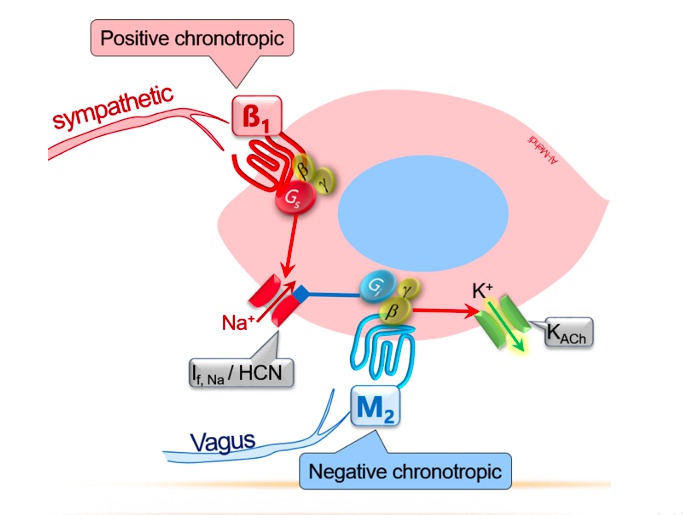
DJ foxglove: digoxin has antiarrhythmic properties
Vegas: digoxin exerts direct parasympathomimetic effects via direct stimulation of the vagus nerve -> (more at) AV nodal inhibition
Irregularly irregular signal: digoxin is useful in atrial fibrillation (and flutter) (1st goal is rate not rhythm)
Metronome: digoxin prevents rapid ventricular response in atrial fibrillation and flutter ("rate control")
Rhythm
if still symptoms after slow rate
synchronized shock, if not can land on T wave = VFIB
reduced risk of converting back

Amigo: amiodarone (class III antiarrhythmic)
"till I die": -tilide suffix shared by dofetilide and ibutilide (class III antiarrhythmics)
Soda: sotalol (class III antiarrhythmic)
Muted bugle: sotalol is also a beta blocker (-lol suffix)
Heart illuminated on top and bottom: class III antiarrhythmics treat both supraventricular arrhythmias and ventricular arrhythmias
Irregularly irregular signal: class III antiarrhythmics treat atrial fibrillation (and flutter)
Converting the signal: class III antiarrhythmics can restore and maintain normal sinus rhythm in atrial fibrillation and flutter

Class IC antiarrhythmics: propafenone, flecainide
Flakes: flecainide (class IC antiarrhythmic)
purple phone: propafenone (class IC antiarrhythmic)
Illuminated top and bottom of heart: class IC antiarrhythmics treat supraventricular and ventricular arrhythmias
Irregularly irregular signal: class IC antiarrhythmics treat atrial fibrillation (and flutter)
Converting the signal: class IC antiarrhythmics can restore and maintain normal sinus rhythm in atrial fibrillation and flutter
spontaneous back to sinus
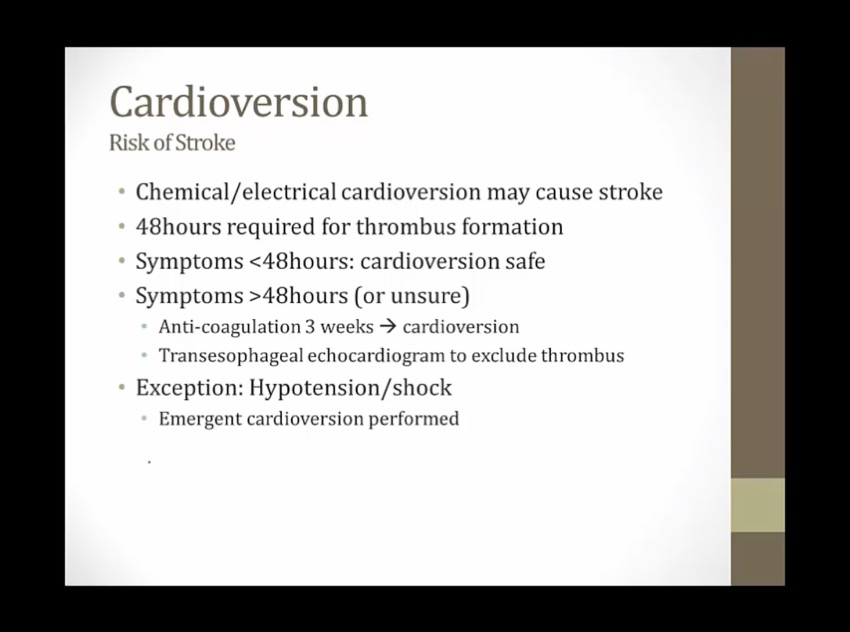
if pt has hypotension/shock with afib: emergent cardioversion
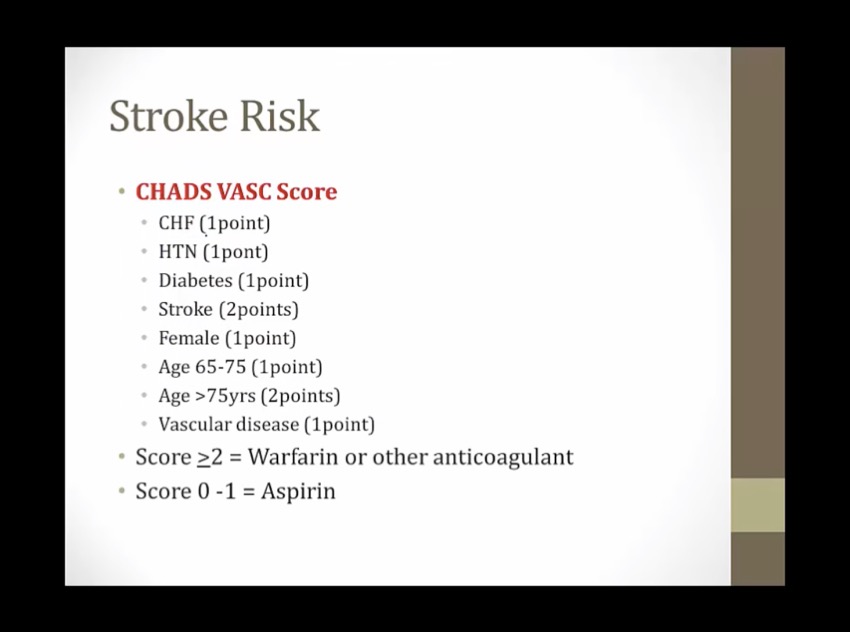
Anticoagulation
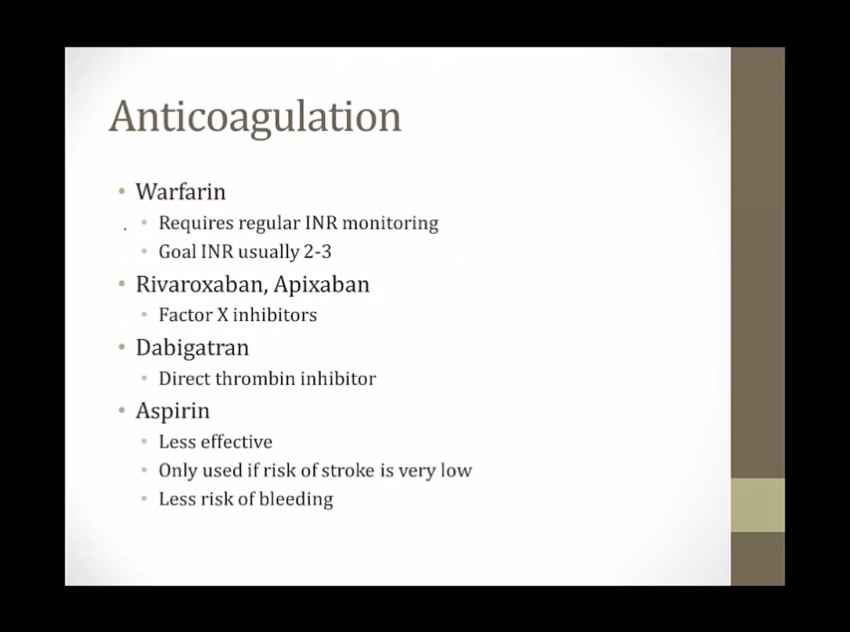

Big GATOR: arGATROban and dabiGATRAN are direct thrombin inhibitors
Banned foXes: direct factor Xa inhibitors rivaroXaBAN and apiXaBAN
Directly grabbing foX: factor Xa inhibitors bind directly
Open mouth: factor Xa inhibitors are oral medications
Irregularly irregular TV signal: direct Xa inhibitors are used for long term anticoagulation in atrial fibrillation

Irregularly irregular signal: warfarin is used for long term anticoagulation in atrial fibrillation. Abnormal heart can increase thrombus formation
even in sinus rhythm, not completely normal atria, some risk of stroke
can have short asymptomatic afib
Surgery
aka afib ablation
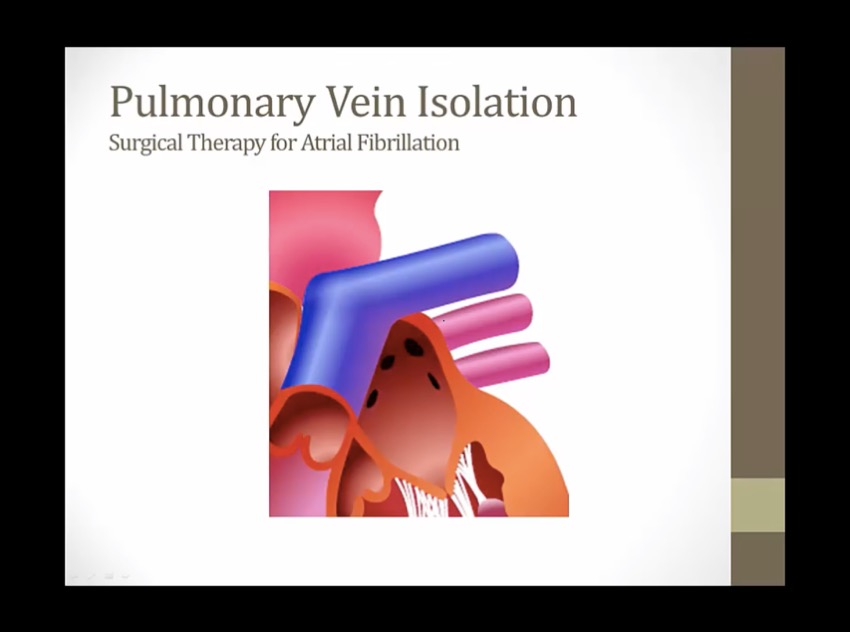
in many cases afib initiated by PA travel to atria
treat afib by catheters that burn myocyte around PA, create small area of nonconducting scar
AFLUT
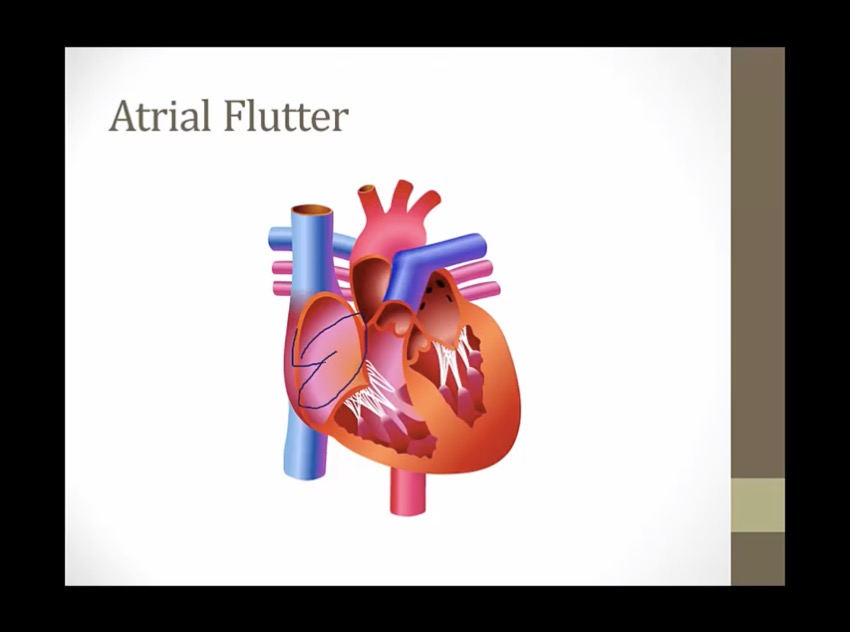
circuit in RA going around and around, each time generate sawtooth pattern, some are conducted to V
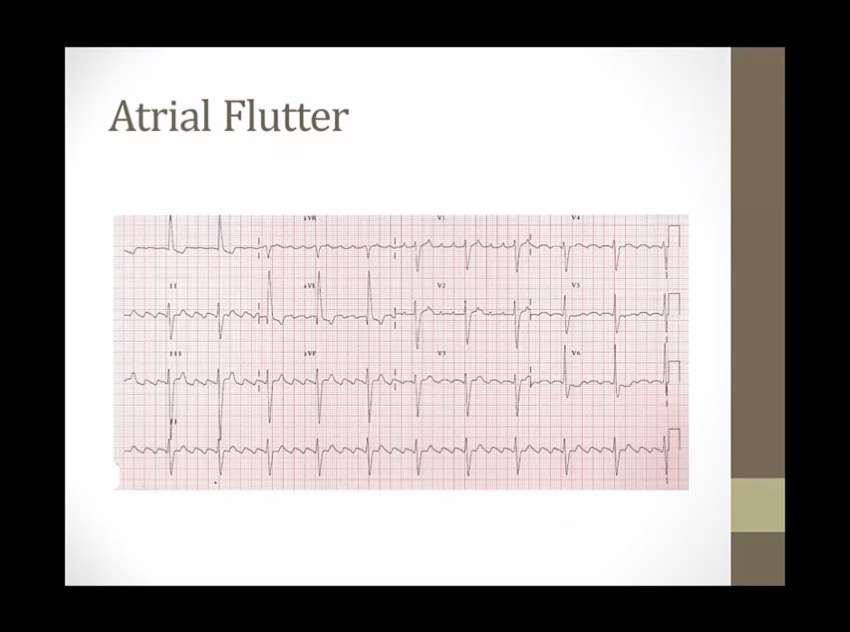
sawtooth EKG
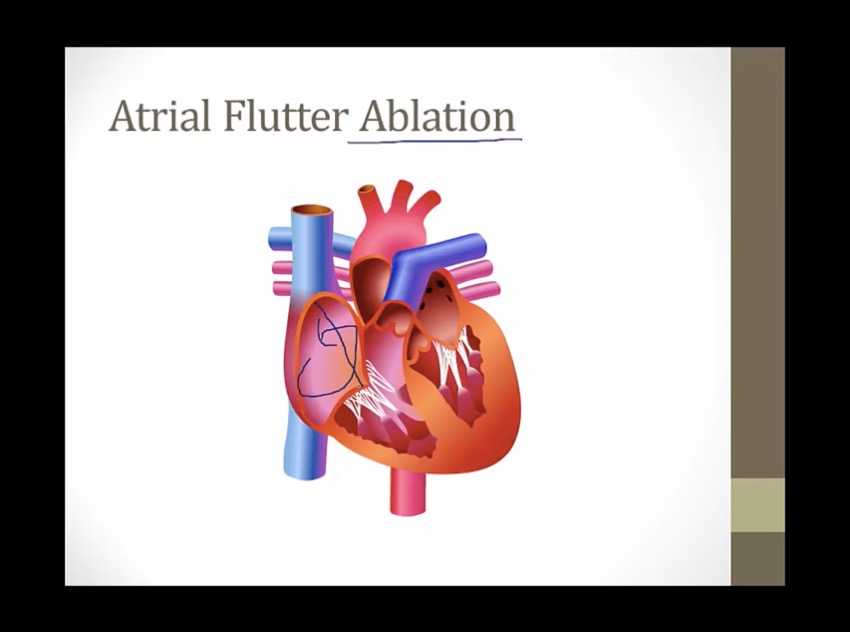
special catheter, burn line of myocyte in atrium, disrupt electrical signal
much easier than AFIB ablation
AVNRT
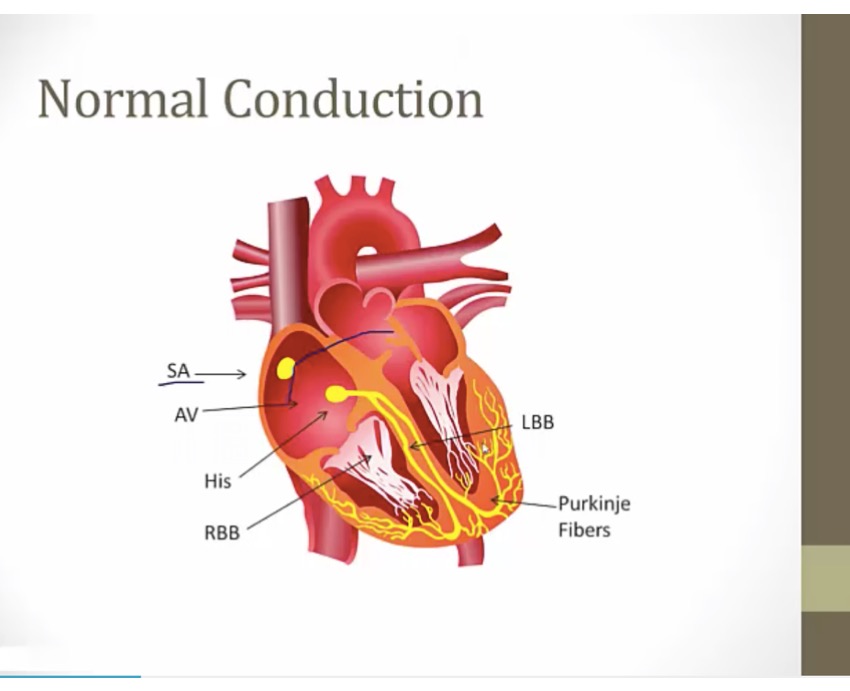
normally: single speed at AV
AVNRT: dual pathways
people develop tissues in AV that conduct at different speed
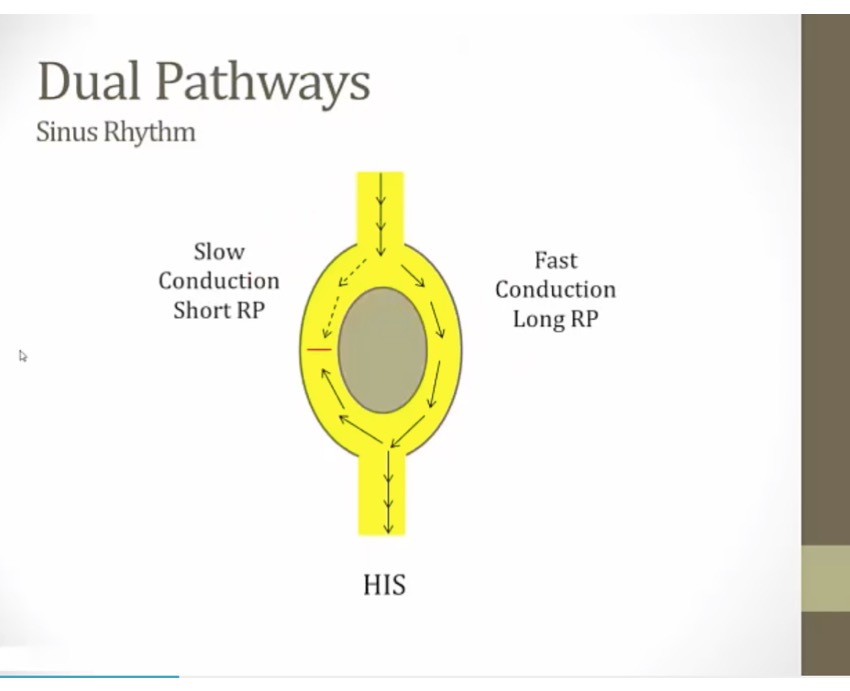
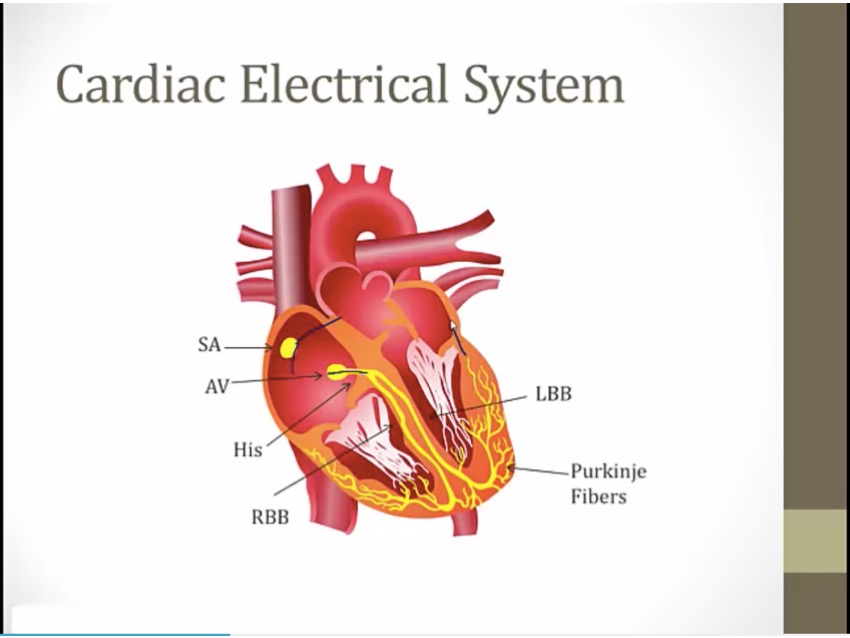
activity comes from SA, splits into slow and fast pathway
fast pathway sends signal down AV and also another one back to slow pathway, cancel out with slow pathway
sinus rhythm: signals cancel out, person asymptomatic
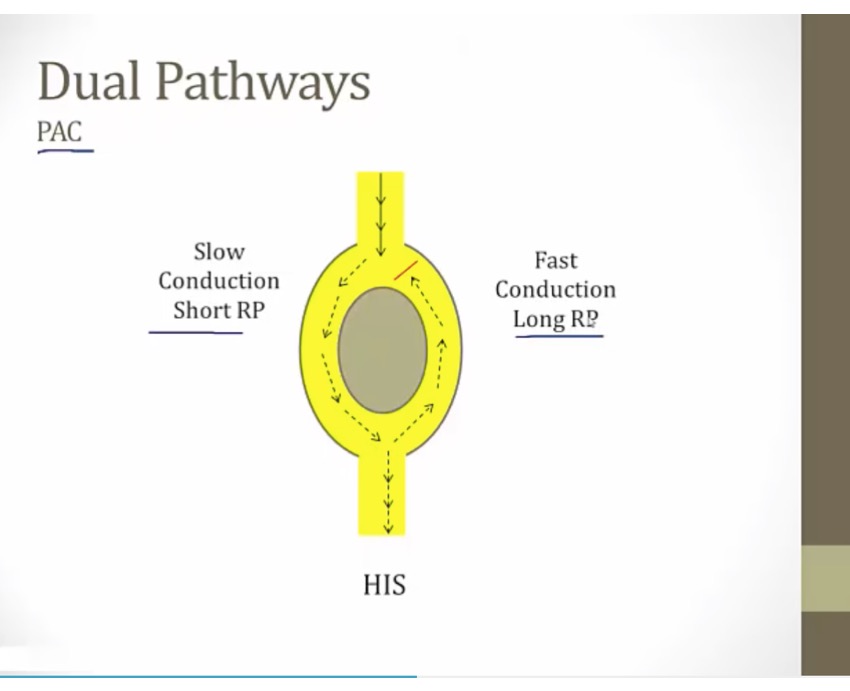
dual pathway and PAC
signal down dual pathway at time when fast pathway is refractory (long RF period)
slow pathway recover quickly
activity go down slow pathway, once reach bottom, fast pathway recovered, so go back up fast and down from slow
result: reentrant circuit, tachycardic rhythm
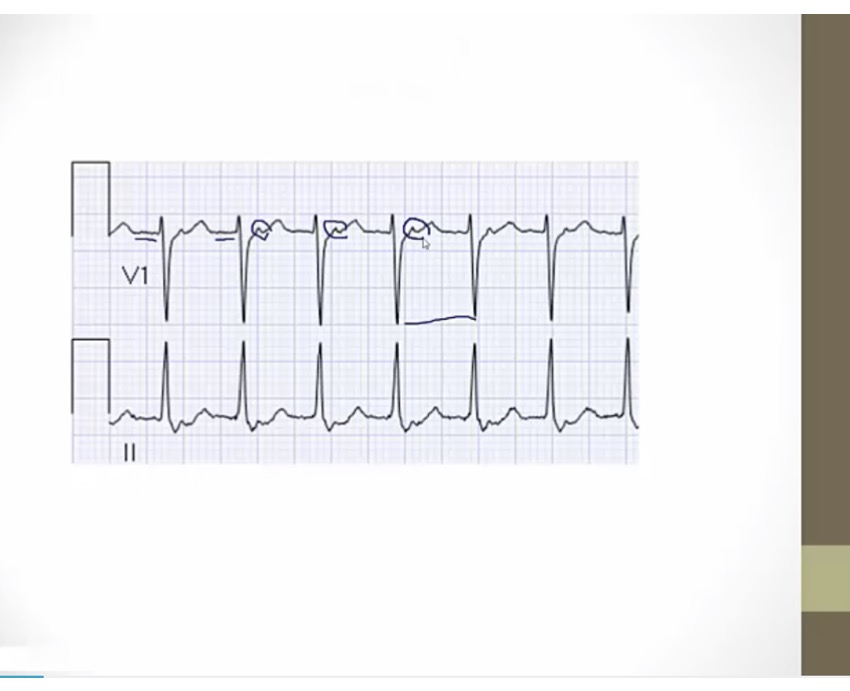
AV nodal reentry tachycardia
no p waves: rhythm generated by AV node
when it comes back up, sends retrograde up to atrium = P wave
narrow QRS: still using AV
fast HR
feel heart pounding
conduction in slow pathway is already slow, if slow down more = block
vagal maneuver: hold breath, slow down heart with increased parasympathetic
adenosine: very flushed and chest discomfort
recurrent: BB, CCB, slow AV
if med fail, surgical
Swing dancing: adenosine (a purine nucleoside with antiarrhythmic properties)
Purine shaped gate: adenosine is a purine nucleotide
A1 Swing: adenosine activates inhibitory A1 receptors on the myocardium and at the SA and AV nodes
Falling calci-yum ice cream: activation of A1 receptors suppresses inward Ca2+ current (hyperpolarization, suppressed Ca2+ dependent AP
Banana flying out of cup: activation of A1 receptors increases outward K+ current (hyperpolarization, suppressed Ca2+ dependent AP)
Note shaped dance floor: adenosine inhibits the AV nodes (decreased AV conduction, prolonged AV refractory period)
Disconnected bottom of heart: adenosine decreases atrioventricular conduction
Dilated coronary crown: adenosine causes coronary dilation (mediated by A2 receptors)
Illuminated #1 top of heart: adenosine is a first line agent for acute treatment of supraventricular arrhythmias (e.g. PSVT)
WPW
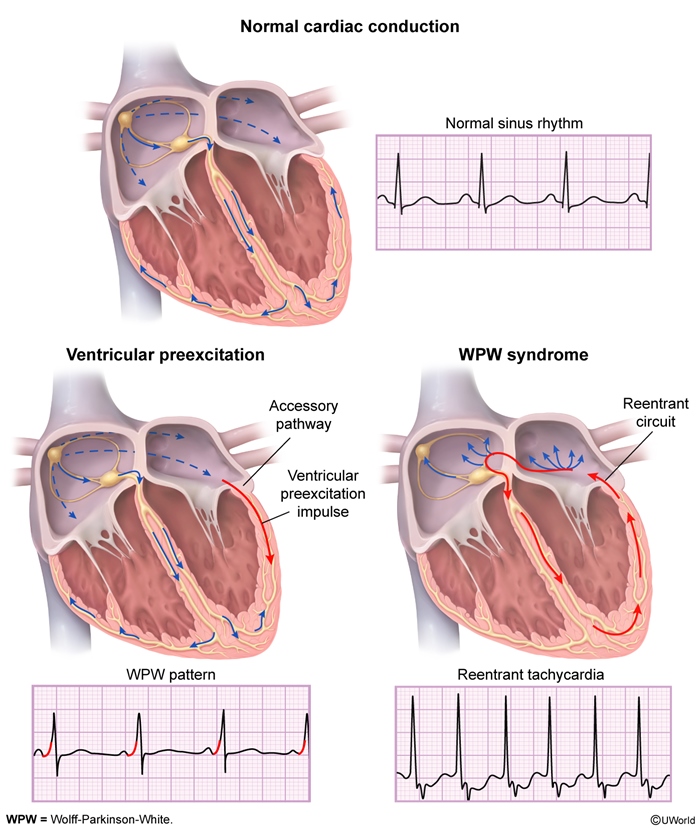
pt: extra piece of tissue (bypass track, white cursor) capable of conducting electricity between atria/ventricles in both directions
electric current will go down AV node but also through atrium to bypass track = early deflection, delta wave
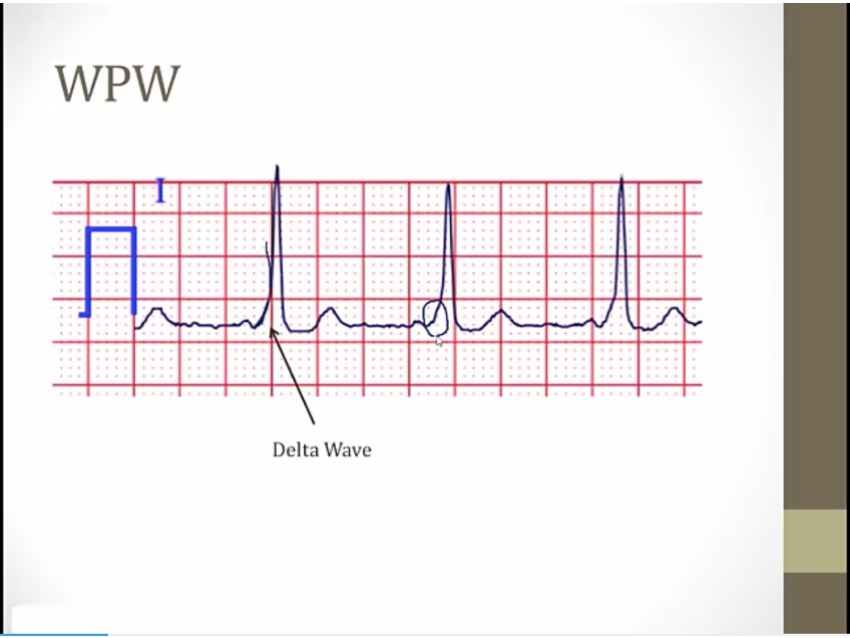
P before every QRS, but QRS begins as soon as P ends
very short PR
inferior lead deep Q
portion at different angle
early activation of ventricle via bypass track
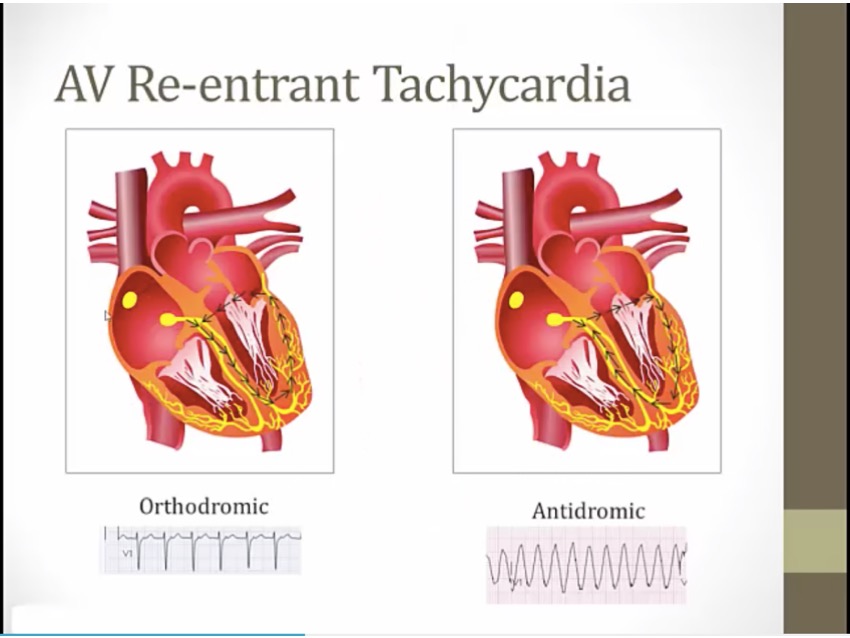
different from AV nodal re-entrant tachycardia
ortho: "correct"
antidromic: go down bypass tract, initiate ventricles abnormally, wide QRS
pattern: asymptomatic
syndrome: symptoms
Illuminated top and bottom of heart: class IA antiarrhythmics treat supraventricular and ventricular arrhythmias
White wolf pack: class IA antiarrhythmics treat Wolff-Parkinson-White (WPW) syndrome (a type of SVT) (extra pathway stopped)
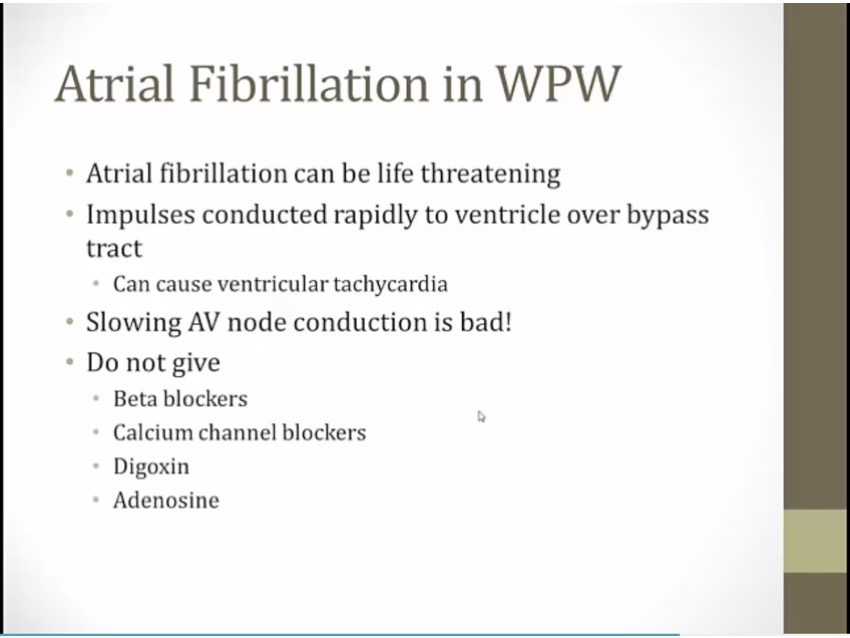
AFIB, if slow conduction through AV node, more impulse sent through bypass tract
highly complex management (electric cardioversion or ibutilide/procainamide). Not important
Last updated